Complete anorectal manometry testing often include the following:
Each of anorectal manometry components is described more fully below.
Anal Sphincter Electromyography (EMG)
Surface Electrode Anal EMG is recording by placing small electrodes peri-anally. The patient then is asked to relax, squeeze and push at different times. The anal sphincter muscle’s electrical activity is recorded using sophisticated computer equipment and displayed on a computer screen. Anal sphincter EMG confirms the proper muscle contractions during squeezing and muscle relaxation during pushing. In people who paradoxically contract the sphincter and pelvic floor muscles, the tracing of electrical activity increases, instead of decreasing, during bearing down to simulate a bowel movement (defecation). Normal anal EMG activity with low anal squeeze pressures on manometry may indicate a torn sphincter muscle that could be repaired.
Anorectal Rest and Squeeze Pressure Profiling
The patient will typically be placed in a semi-recumbent position, and a 4-channel radial air-charged anorectal catheter will be inserted approximately 4 cm into the rectum. The catheter will be slowly withdrawn at one centimeter intervals as resting and squeeze pressures are recorded in 4 quadrants (Anterior, Right, Posterior and Left). Average resting pressure is recorded using the advanced diagnostic equipment. Above 40 mmHg is normal for resting pressure. Also, average squeeze pressure will be recorded. Greater than 100 mmHg is normal for average squeeze pressure. Anal canal length is also typically measured. Normal anal canal length is 3 to 4 centimeters. Figure 2 below shows both the average and maximum pressure measurements and how they would typically appear on a complete anorectal manometry summary report.
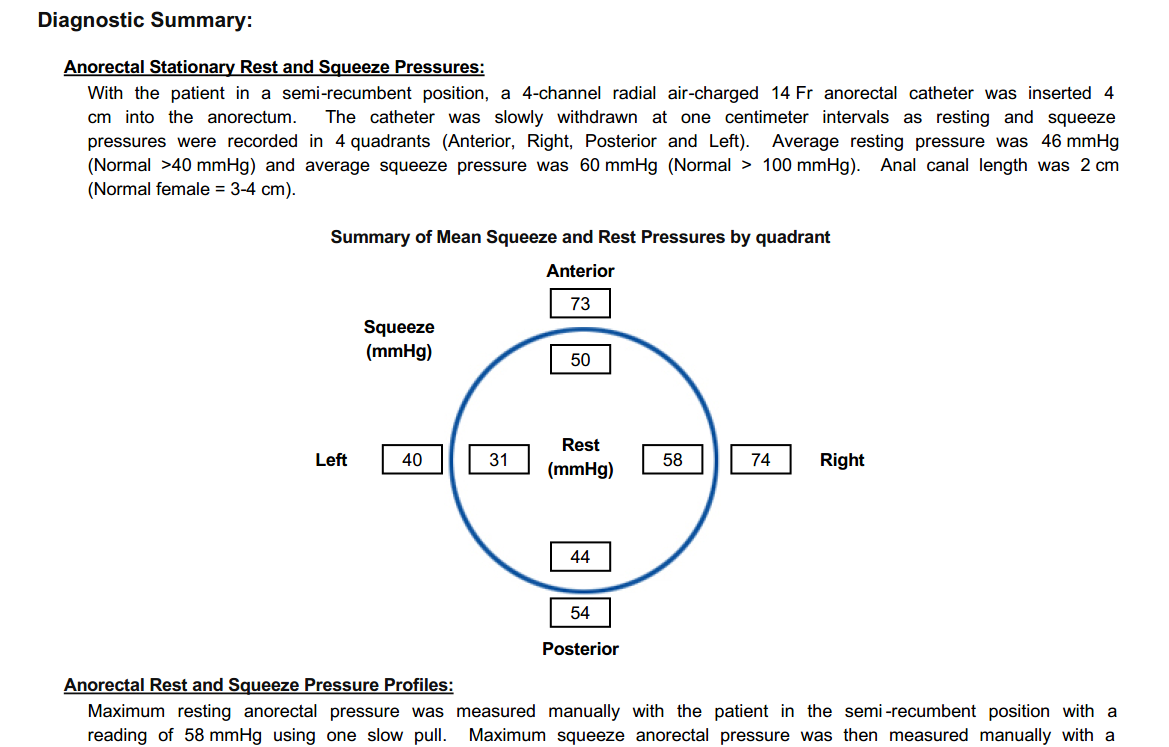
Figure 2 - Anorectal Manometry Rest and Squeeze Pressure Profile Example
Rectal Volume Measurement
With the patient in a semi-recumbent position, the inserted rectal balloon will be slowly filled with water to assess and record the following rectal sensations: first sensation of rectal filling, first urge to defecate, and maximum tolerable rectal volume. For a normal patient, the first sensation will normally be reported between 10 and 60 milliliters; the first urge to defecate should manifest at 10 to 100 milliliters of filling; and the maximum tolerable rectal volume will range from 200 to 300 milliliters.
Rectoanal Inhibitory Reflex Measurement
The rectoanal inhibitory reflex is a response of the internal anal sphincter to rectal distention. The transient relaxation of the internal anal sphincter in response to rectal distention plays an important role in the continence mechanism. During the anorectal manometry test the patient will be placed in a semi-recumbent position and the rectoanal inhibitory reflex will be assessed as the water or air-filled catheter is inflated. A normal reflex should occur between 10 and 30 milliliters.
Balloon Expulsion Test
The balloon expulsion test provides an assessment of the patient's ability to evacuate artificial stool during simulated defecation within the laboratory environment. For the balloon expulsion test, a small balloon (as seen above in Figure 1) is inserted into the rectum and then inflated with approximately 50 ml (2 ounces) of water or air, and the patient is asked to expel it into a toilet. The patient goes to the bathroom and tries to defecate (expel) the small balloon from the rectum. The amount of time it takes to expel the balloon is recorded. Prolonged balloon expulsion suggests a dysfunction in the anorectal area.
Procedure Summary
The test takes approximately 30 to 45 minutes. The patient must change into a hospital gown. A nurse will explain the procedure thoroughly to the patient, take a brief health history, walk the patient through a fecal incontinence and constipation related health questionnaire, and answer any questions the patient has. The patient then lies on his or her left side. A small, flexible tube, about the size of a thermometer, with a balloon at the end is inserted into the rectum. The catheter is connected to the electronic manometry equipment that measures the pressure. During the test, the small balloon attached to the catheter may be inflated in the rectum to assess the normal reflex pathways and muscle response.
The nurse will also ask the patient to relax, squeeze, and push at various times. The anal sphincter muscle pressures are measured during each of these muscle contraction/relaxation actions. To squeeze, the patient tightens the sphincter muscles as if trying to prevent anything from coming out. To push or bear down, the patient strains down as if trying to have a bowel movement.
Two additional tests will also be done as part of the full anorectal manometry group of diagnostics. An anal sphincter electromyography (EMG), a test to evaluate the nerve supply to the anal muscle, and the measurement of the time it takes to expel a balloon from the rectum, both described more fully above.
The anorectal manometry testing requires no anesthesia, so you will be able to go about your normal activities after the test. The full interpretation of all the data takes considerable time and review by the physician. Therefore, your physician may not have the test summary for several days.